IV. RESULTS AND DISCUSSION
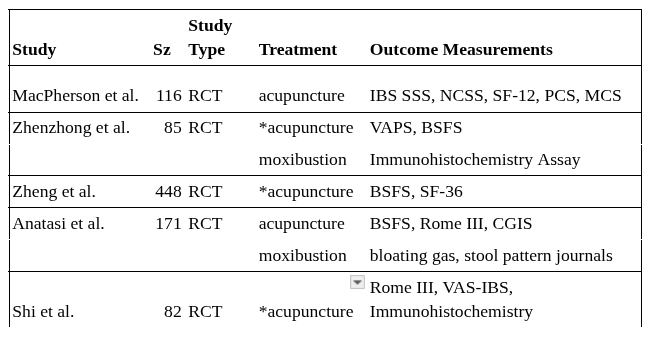
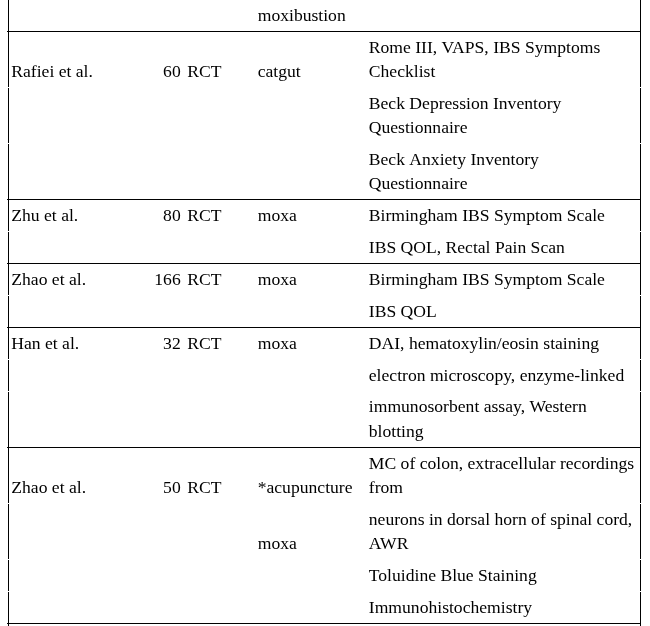
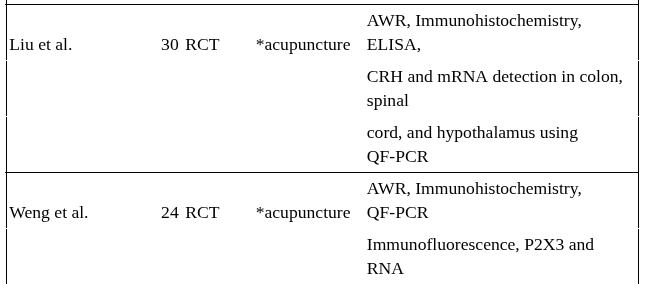
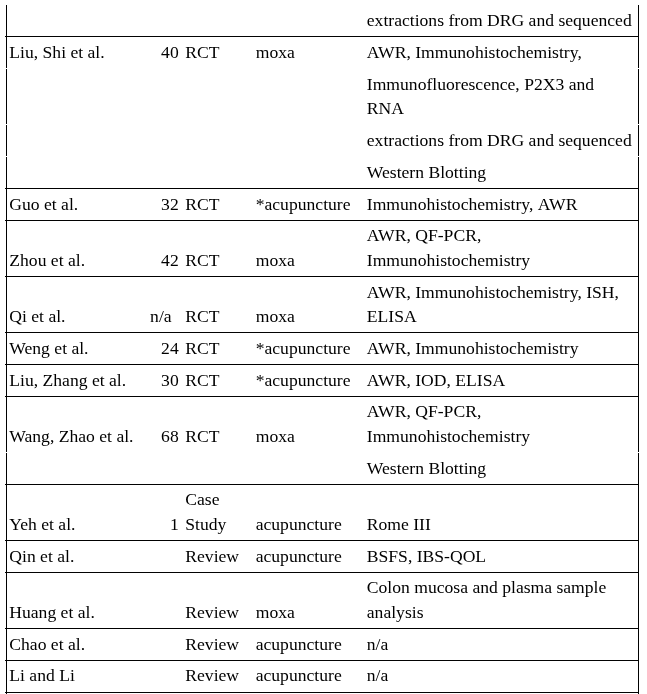
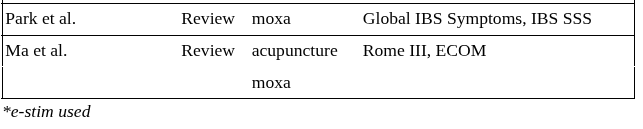
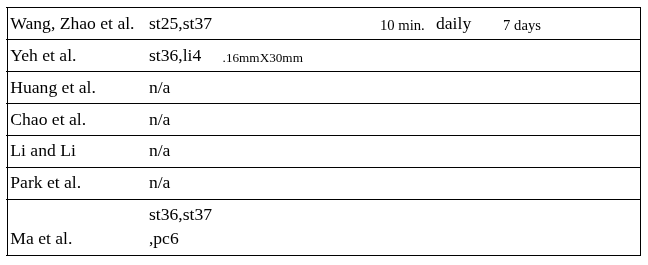
Sample sizes varied greatly between studies. The majority of the studies had sample sizes with less than 100 subjects and none of the studies had sample sizes greater than 500 subjects. Greater sample sizes produce more robust clinical trials and reviews which is a point for future research efforts to consider. The outcome measurements, which are the most important features to mark treatment success, were also highly variable. Many of the outcome measurements were subjective, which allowed for variability in interpretation. This inconsistency made the summarization of data more challenging. Table 1 shows sample size, study type, treatment, & outcome measurement.
Table 1. Sample Size, Study Type, Treatment, & Outcome Measurement
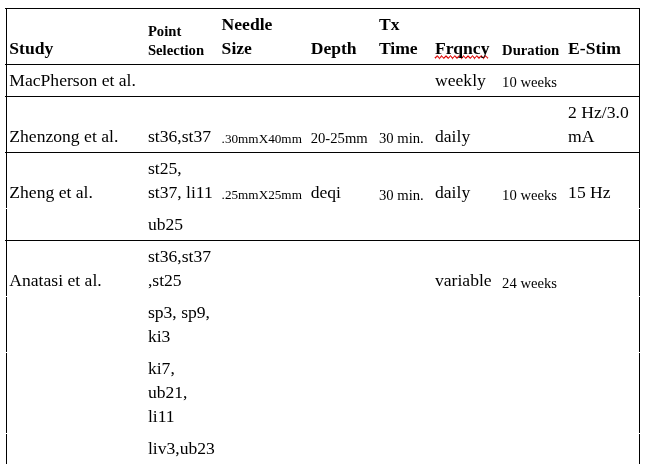
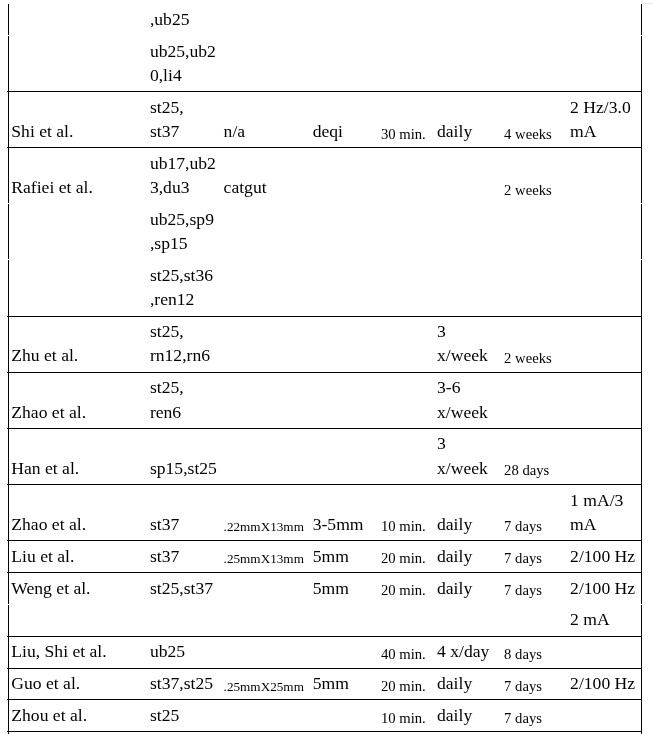
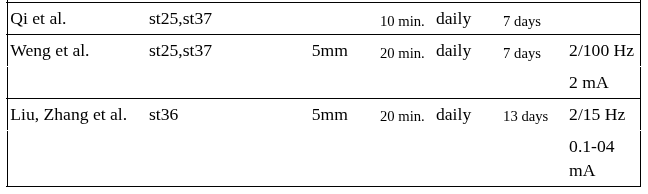
In the RCTs, the details on how the treatments were performed also lacked consistency and transparency. Missing information regarding treatment strategies made it difficult to accurately compare extracted data. Many of the the studies lacked treatment details regarding needle type, needle depth, duration of treatment, or frequency of treatment. In order to build a solid case for any treatment model, the exact details of the treatments need to be disclosed. Table 2 shows treatment strategies while figure 4 shows the ratio of trials using acupuncture only, moxibustion only, and the combination of acupuncture and moxibustion.
Table 2. Treatment Strategies
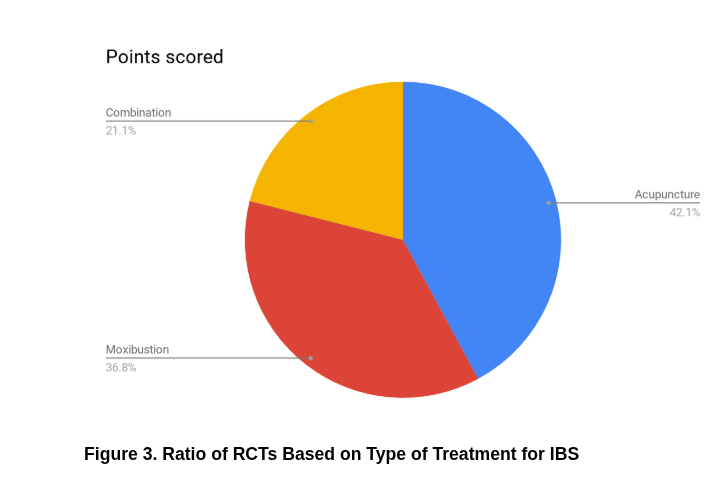
The statistical significance scores provided the ability to analyse treatment models and compare effectiveness. It was established that the combination of both moxibustion and acupuncture used together outperformed the use of acupuncture and moxibustion used separately. Table 3 shows the statistical significance values for each study. Figure 4 shows the comparison of the scores based on statistical significance, sample size, quality of review, and outcomes that were considered positive.
Table 3. Statistical Significance
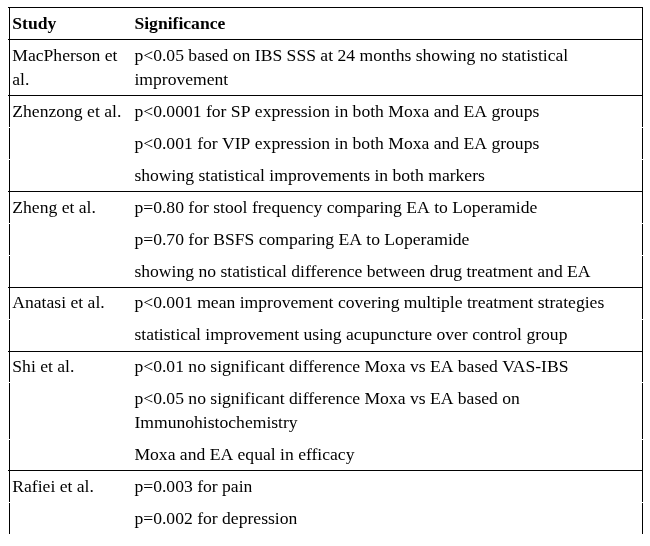
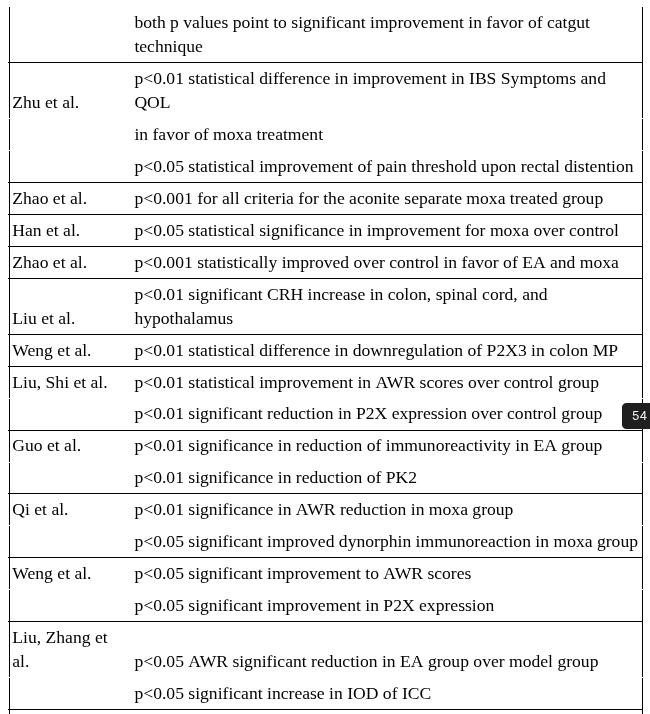
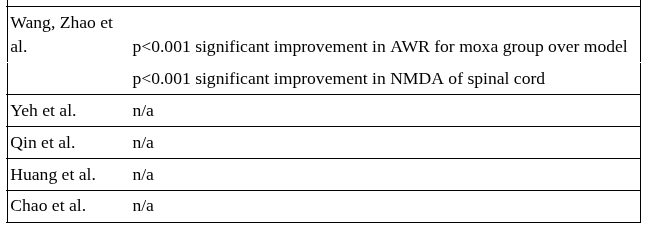
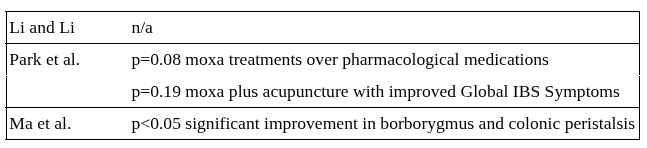
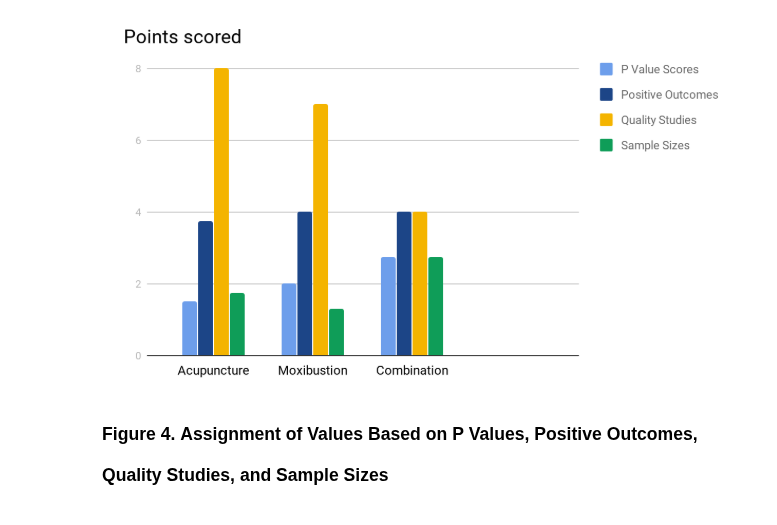
Figure 4 was designed based on values given to extracted data using a generalized point averaging scale. Points were awarded based on p value scores, number of outcomes that were considered positive by the authors (including subjective and objective scoring, regardless of statistical significance), number of peer reviewed RCTs, and sample sizes. Scores were tallied and averaged based on the number of studies in each category.
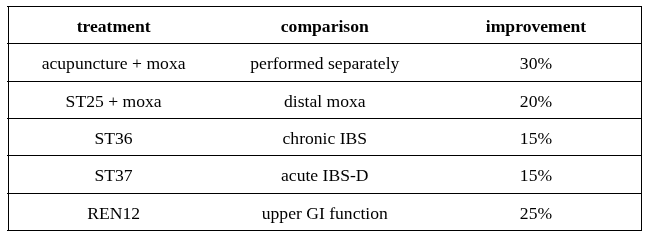
ST25, ST36, ST37, and REN12 performed better for IBS related symptoms over any other acupoints used in the studies. Table 4 shows the percent to which the acupoint performance excelled. The combination of moxibustion and acupuncture is also listed as performing better when used together than when used separately.
Table 4. IBS Acupoint & Treatment Performance
Randomized Controlled Trials (Human Subjects)
Clinical Study #1
In the study by MacPherson et al., the main outcome measurements were based on the IBS SSS, NCSS, PCS, MCS, and the SF-12 (see Appendix A). The aim of the study was to follow up on a prior study with a 24 month post-randomization clinical trial. Two major limitations of the trial were the heavy reliance on lifestyle changes based on the initial treatments (first trial), direction given to the patients by the acupuncturists, and missing data (61% of the participants provided completed IBS SSS data). As a result, the adjusted difference between the means at 24 months was not statistically significant with the exception of NCSS and IBS SSS scores at 3 months (p<0.05). The lack of statistically significant treatment effect at 24 months could be due in part to the small size of the remaining sample, and the concurrent progressive reduction in IBS symptoms in the usual care group after 12 months. The strength of this study is that it attempts to address the value of continued treatment. Since it is assumed that much of the impact of AOM treatments are cumulative, studies that assesses long term vs short term treatments are important and currently lacking. This study could be used in the future to justify maintenance programs. The weakness of this study is the declining sample size combined with high variability in treatment approaches with uncontrolled lifestyle factors.
Clinical Study #2
In the study by Zhenzhong et al., SP expression in the colonic mucosa was significantly reduced for IBS-D and IBS-C patients in both EA and Moxa groups (p<0.0001). There was no significant difference in outcomes between those two groups in treating IBS-D indicating that both EA and Moxa are effective treatments; however, there was a significant difference in treating patients with IBS-C. EA was more effective in reducing over-expression of SP in colonic mucosa (p<0.024) over moxa (p<0.05). VIP expression in colonic mucosa was significantly reduced (p<0.001) in both the moxa and EA groups after treatment. There was no significant difference between the Moxa and EA groups in treating IBS-D; however, there was a significant difference in the EA group (p<0.001) in treating IBS-C patients over the control group. Based on the VAPS, both the Moxa and EA groups experienced significant pain reduction from treatment (p<0.0001) however, the moxa group showed a significant improvement over the EA group (p<0.001). The authors concluded that EA and Moxa treatments were both effective in treating IBS symptoms; however, they recommend Moxa for IBS-D and EA for IBS-C. The strength of this study is the differentiation between the use of moxibustion vs acupuncture in efficacy for treating different patterns of IBS. In the future this study could be used to justify one treatment over another based on the individual needs of the patient.
Clinical Study #3
Zheng et al. divided a total of 448 participants randomly into 4 groups. 3 groups for acupuncture treatment using different acupoints and the remaining group treated with a Loperamide. There was no significant difference in stool frequency between the four groups (p=0.80) at the end of treatment and no significant difference in BSFS (p=0.07). Study showed that electroacupuncture was equivalent to Loperamide in treating IBS-D or functional diarrhea. The strength of this study is the large sample size and the comparison to drug treatment. In the future, this study may be used to justify acupuncture as an alternative treatment option over drug based treatments for IBS.
Clinical Study #4
Anatasi et al. used diagnostic patterns to decide acupoint prescriptions which let to high variation in treatment strategies and goals. The outcomes were based on reduction of pain and IBS secondary symptoms (bloating, gas, and stool consistency) that were recorded using daily journals and weekly clinical global impression scale. Overall the study showed mean statistical improvement (p<0.001) justifying further research (this was a pilot study). Individuated treatments decreased reproducibility and rely on practitioner experience to diagnose and select acupoints based on skill making this study less useful in a conventional care environment. This study is useful as it was one of the only studies that differentiated IBS through the AOM diagnostic patterns of IBS. In the future the eight patterns of diagnosis may be used in studies for individualized care, which is the cornerstone of AOM treatments. The weakness of this study in using diagnostic patterns is that reproducibility goes down.
Clinical Study #5
Shi et al. created their study to determine the difference in efficacy between Moxa and EA in treating patients with IBS. Based on the VAS-IBS and immunohistochemistry assay there was no statistical significant difference (p<0.01 and p<0.05 respectively). However, they did detail a general advantage of EA in treating IBS-C and Moxa in treating IBS-D. The strength of this study is the detailed strategies using moxa and EA treatments. This study provided specific applications that will be duplicated in the future for treatment efficacy.
Clinical Study #6
The research by Rafiei et al. showed statistical significance in the areas of pain and depression in IBS patients using catgut acupuncture technique over sham acupuncture and drug-only treatments (p=0.0003, P=0.0002 respectively). Four main areas of assessment (symptoms, pain, depression, anxiety) all improved but only pain and depression showed statistical significance. The strength of this study was the prescreening of patients and exclusion of illnesses (and related medications) that could influence outcomes. It is valuable for future practices and research because the catgut technique is relatively new and there is little supportive data although the application is promising. This technique is nonexistent in the United States and, in the future, this study will help to introduce catgut acupuncture into the medical system of the United States. The weakness of this study is the number of acupoints chosen which increases variability and makes duplication difficult.
Clinical Study #7
Zhu et al. induced moxibustion analgesia in their study. Their results were in favor of moxibustion as a treatment strategy for IBS. Birmingham IBS Symptom Survey numbers along with quality of life assessments showed statistically significant improvements (p<0.01). The subjects were also given colorectal irritation through ballooning. The pain threshold of the moxibustion group improved significantly over the control group (p<0.05). In the authors’ conclusion, they noted (without statistical significance) that moxibustion decreased activation of the prefrontal cortex and the anterior cingulated cortex. The strength of this study is the assessment of brain functions affected by moxibustion related to IBS. The weakness of this study is the use of an herbal barrier when applying moxibustion. The herbal barrier introduces an uncontrolled treatment variable which makes differentiation of response mechanisms difficult.
Clinical Study #8
Zhao et al. showed us that aconite-separated moxibustion group resulted in significantly lower scores (improved) (p<0.001) after the first and second treatments. The study concluded that aconite-separated moxibustion therapy applied three times per week with one cone per application was an effective treatment for patients with IBS. The aim of this study was to examine the effect of moxibustion with an herbal barrier (unlike clinical study #7). This becomes a strength as future practices may include herbal barriers when treating with moxibustion.
Randomized Controlled Trials (Animal Subjects)
Clinical Study #1
Han et al. used light and electron microscopy to show neatness of glandular arrangement in colonic mucosal epithelia. DAI has been widely used for evaluation of disease activity and allowed the integration of various aspects of disease into a single value. DAI scores were significantly improved over the control group (p<0.05) in favor of moxibustion for the treatment of IBS. Treatments were given in 3, 6, and 9 minute intervals in which the authors implied that the 9 minute treatments were more beneficial. The strength of this study is the distinction of treatment times using moxibustion. In the future, this information can be used in practice to increase efficacy based on length of time treated.
Clinical Study #2
Zhao et al. showed evidence that EA performed with different intensities on ST37 increased activation effects on WDR neurons in the dorsal horn of the spinal cord in model rats with visceral hypersensitivity at a level of statistical significance (p<0.001). Moxibustion treatments were found to be superior over the EA treatments. Mast cell degranulation rates in the colon were also increased in the moxibustion and EA groups compared to the control group. The dorsal horn of the spinal cord is the key to regulation of visceral hypersensitivity and it is clear, from this study, that moxibustion and EA can inhibit the response of the neurons in the dorsal horn of the spinal cord activated by visceral nociceptive afferent impulses. The strength of this study is the comparison between acupuncture and moxibustion and the outcome assessments which included the brain-gut axis. In the future this study can be used to choose either acupuncture or moxibustion based on the individual needs of the patient.
Clinical Study #3
Liu et al. performed research showing electroacupuncture was able to significantly reduce the visceral hypersensitivity in rats and regulated the expression of corticotropin-releasing hormone (CRH) protein and mRNA in the colon playing a role in the model of irritable bowel syndrome (p<0.01). The strength of this study is the examination of CRH. This outcome value is useful to support the relationship of the brain and the gut in IBS patients. This study could be used in the future to justify IBS treatments that are aimed at the brain for decrease of visceral hypersensitivity.
Clinical Study #4
Weng et al. used abdominal withdrawal reflex scores to assess progress along with immunofluorescence and immunohistochemistry to measure P2X3 receptor expression in the myenteric plexus neurons. EA showed statistical significance in improving downregulation of P2X in myenteric plexus (p<0.01). The strength of this study is the assessment of purinergic receptor function in relation to acupuncture treatments. This information can be used to justify future studies focused on the nervous system and hormone system for the treatment of IBS using acupuncture.
Clinical Study #5
Liu, Shi, et al. used immunohistochemistry, RNA preparation and reverse transcriptase, and Western blotting markers. Observations from the double immunofluorescence staining analysis showed that the co-expression levels of P2X7 receptors was significantly increased compared to the rats in the control group (p<0.01). The strength of this study is the examination of the DRG in outcomes. This study can be used in the future to justify further research on the nervous system for the treatment of IBS patients using moxibustion.
Clinical Study #6
Guo et al. attempted to reduce P2X4 receptor expressions in subjects with visceral hypersensitivity. After treatment, the rats from the electroacupuncture group showed a significant reduction in abdominal reflex scores (p<.05) and showed similar scores as the rats treated with intragastric administration of pinaverium bromide (p<.05). Immunohistochemistry revealed that P2X4 receptor immunoreactivity was significantly lower in these same two groups (p<0.01). Immunoreactivity was also shown to be lower in the spinal cord. The strength of this study is the comparison of AOM treatments to drug based treatments. In the future, this study can be used to justify giving patients an alternative to drug treatments for IBS.
Clinical Study #7
Zhou et al. performed a randomized controlled trial showing moxibustion therapy reduced AWR scores of rats at all intensities (20 mmHg, 60 mmHg, and 80 mmHg) significantly (p<0.01). They also determined the effects of moxa treatment on the expression of PK2 and showed a significant decrease (p<0.01). The strength of this study is the specificity in which the moxibustion treatments were described. The details in application, from this study, can be used in future patient care when moxibustion is indicated.
Clinical Study #8
Qi et al. performed a randomized controlled trial using warming moxibustion therapy to treat chronic visceral hyperalgesia in rats. Levels of dynorphin showed a significant response from warm moxibustion treatment (p < 0.05) and AWR reduced over model group (p<0.01). The strength of this study is the measurement outcomes based on the dynorphin system. The influence of moxa therapy on this particular mechanism of function is poorly researched. This study will allow for more research to be done in this area.
Clinical Study #9
Weng et al. used immunohistochemistry to detect P2X receptor expression in dorsal root ganglia from rats with chronic visceral hypersensitivity and recorded a statistically significant improvement over the model group (p<0.05). They also documented significant improvement (p<0.05) in AWR scores using electroacupuncture. The uniqueness and strength of this study is the specific use of ST37 and ST25, with measurable effects, on the purinergic receptor system. This is both useful clinically as well as justifies further research on this topic.
Clinical Study #10
Liu, Zhang, et al. performed a randomized controlled trial to identify changes in the interstitial cells of Cajal (ICC) in rats with chronic psychological stress through electroacupuncture treatments on ST36. They recorded significant improvements in AWR and ICC scores (p<0.05). The strength of this study is both that it incorporates psychological stress, which is an important contribution to pathogenesis, and the uniqueness of the outcome measurement of interstitial cells of Cajal. This study will support future research on both psychological and biological stress factors related to IBS.
Clinical Study #11
Wang, Zhao et al. , Huang, and Tan performed a randomized controlled trial using moxibustion therapy to treat IBS. After moxibustion treatment, the abdominal withdrawal reflex scores were significantly improved (P<0.001). Detection of NMDA in the spinal cord using western blot showed increased expression in the model group compared to the normal group (P< 0.001). Moxibustion treatment both downregulated NR1 and NR2B proteins in the spinal cord (P<0.05). These results suggest that the expression of NR1 and NR2B protein significantly increases in the spinal cord of IBS visceral hyperalgesia rats and that moxibustion on ST25 and ST37 reverses this increase.
Case Study
Yeh et al. did a case study on the treatment of IBS in an 11 year old girl to suggest integrative care models for treatment of pediatric patients with gastrointestinal diseases and disorders. Although the patient showed clinical benefits from the acupuncture treatment there was no method for extracting statistical significance. The research team felt very strongly that acupuncture was clinically effective at treating IBS however, the acupuncture treatments were combined with dietary changes, herbal medicines, nutritional supplements, acupressure, and magnet therapies which limits the ability to gauge the efficacy of the acupuncture treatments. The weakness of this case study is that too many other modalities were combined within the treatment approach making it impossible to assign efficacy values.
Systematic Reviews and Meta-Analysis
Qin et al. performed a systematic review with mixed results were mixed. Some studies reported that acupuncture was more effective than sham acupuncture and some studies reported that it was not more effective (statistical analysis not available). The conclusion of the review was that more Randomized Controlled Trials were needed to prove clinical effectiveness.
Chao et al. performed a meta-analysis on the effectiveness of acupuncture in treating patients with irritable bowel syndrome. The analysis of six randomized controlled trials suggests that acupuncture improves the symptoms of IBS. However, the data was insufficient to recommend acupuncture as first-line treatment.
Park et al. detailed mixed results on the performance of moxa therapy as a medical treatment for IBS. While some of their reviewed studies showed statistical improvements (p=0.08) other studies showed no statistical improvements (p=0.10). The conclusion was that the authors were unable to support moxibustion as evidence-based medicine.
Qualitative Reviews
Huang et al. performed a literature review to evaluate the mechanisms of effect in the application of moxibustion for analgesia with patients that suffer irritable bowel syndrome. The group concluded that that mechanisms of treatment effects on IBS involve a number of organs and targets; however, relevant studies were from different points of view and current systematic and comprehensive research is still lacking. No data on statistical analysis is available.
Li and Li reported that acupuncture was effective at treating IBS and quoted a total effective rate at 90.48% in the acupuncture group compared to 78.95% in the medications group. The report concluded that acupuncture was effective medically while at the same time reduced in cost over conventional care; however, statistical analysis was not provided.
Ma et al. reviewed treatments that showed statistically significant improvements in borborygmus frequency and colonic peristalsis (p<0.05). These results indicated that acupuncture can immediately regulate colonic peristalsis in patients with IBS-D using ST36 and ST37. However, the authors concluded that the variety of treatment strategies using acupuncture and moxibustion make it impossible to study the complex and comprehensive issues related to the action mechanisms.